





 Podcast
Podcast Sign Up
Sign Up Virtual Learning
Virtual Learning Online CEUs
Online CEUs Streaming Video Library
Streaming Video Library
Exploring Risk Factors and Implications of Age
By Ehud Yairi, Ph.D.
University of Illinois
 Age is among the strongest risk factors for stuttering with several important implications. Although the disorder begins within a wide age-range, current robust evidence indicates that, for a very large proportion of cases, it erupts during the preschool period. Data obtained at the University of Illinois Stuttering Research Program revealed that for 65% of the child participants, stuttering onset occurred prior to age 3; the figure rose to 85% by 3 1/2 years of age (Yairi & Ambrose, 2005). Leaving room for some sampling errors, children past age 4 face a relatively low risk for stuttering. From clinical considerations, these statistics call for greater emphasis on preparing clinicians for working with early childhood stuttering.
Age is among the strongest risk factors for stuttering with several important implications. Although the disorder begins within a wide age-range, current robust evidence indicates that, for a very large proportion of cases, it erupts during the preschool period. Data obtained at the University of Illinois Stuttering Research Program revealed that for 65% of the child participants, stuttering onset occurred prior to age 3; the figure rose to 85% by 3 1/2 years of age (Yairi & Ambrose, 2005). Leaving room for some sampling errors, children past age 4 face a relatively low risk for stuttering. From clinical considerations, these statistics call for greater emphasis on preparing clinicians for working with early childhood stuttering.
Age brings out other factors. The fact that the critical age for stuttering onset parallels the age span when significant rapid developments occur in the anatomy of the speech system, as well as in complex language and articulatory skills, invites speculations that interferences in these maturational processes contribute to stuttering; hence the possibility of relations among stuttering, language, and articulation. Although our own data (Watkins, Yairi, & Ambrose, 1999), and those of our colleagues from Germany (Rommel et. al., 1999), show that the language skills of children who stutter, as a group, meet or exceed norms, we suspect that there are differences in the ways in which they process language. One research priority consequent to information about age at onset is experimental manipulation of similarities and/or differences in language processing and production between children who stutter near the onset of the disorder and normally fluent children, particularly in terms of the nature of linguistic knowledge and the time course of knowledge activation. Varied responses to semantic and phonological distracters, slower reaction time, and/or alternative activation paths may reveal differences in language processing. One of the intriguing questions is: does age at stuttering onset — prior to, or after, a certain point in language development — underlie distinct subtypes of the disorder? Unfortunately, only a few scientists have been interested in the subtypes issue, e.g., Seery, et al. (2007) and SheikhBahaei, et al. (2023).
Brain imaging studies of young children should also continue to enhance understanding of the age factor. Years ago, our team members, Chang, Erickson, and Ambrose (2005) successfully obtained high resolution structural MRI data from stuttering and control children ages 8-13. Their initial results indicated significant group differences in white and grey matter volume in brain areas involved in integrating sensory and motor aspects of speech. Certainly, the younger the children, and the closer to onset they are, will advance our knowledge about the etiology of the disorder.
There is some evidence that age at onset may bear a relation to genetic factors, in particular there seems to be a trend for persistent stuttering to have a slightly later onset than recovered stuttering (Yairi & Ambrose, 2005). This, however, appears to be complicated-and as a large recent study found 57 genomic regions that mapped to 48 genes associated with stuttering (Polikowski et al., 2025).
 Age is also a risk factor in regard to children's awareness of disfluent speech. The belief that preschoolers who stutter lack in such awareness played a major role in theories and developmental models of the disorder. For many years, clinicians' assumption that awareness would trigger strong emotions (e.g., anxiety) in children was the main reason for shunning direct speech therapy for preschoolers. Whereas some three-year olds are either clearly, or appear to be, aware of stuttering, available experimental data show a very large increase in awareness between ages 4 and 5, including normally fluent children (Ambrose & Yairi, 1994; Ezrati, Platzky, & Yairi, 2001). This information would seem to justify direct intervention techniques as well as provide clues for the timing of intervention and should be considered in counseling of parents and teachers about reactions of normally fluent children to their stuttering peers.
Age is also a risk factor in regard to children's awareness of disfluent speech. The belief that preschoolers who stutter lack in such awareness played a major role in theories and developmental models of the disorder. For many years, clinicians' assumption that awareness would trigger strong emotions (e.g., anxiety) in children was the main reason for shunning direct speech therapy for preschoolers. Whereas some three-year olds are either clearly, or appear to be, aware of stuttering, available experimental data show a very large increase in awareness between ages 4 and 5, including normally fluent children (Ambrose & Yairi, 1994; Ezrati, Platzky, & Yairi, 2001). This information would seem to justify direct intervention techniques as well as provide clues for the timing of intervention and should be considered in counseling of parents and teachers about reactions of normally fluent children to their stuttering peers.
From early on, age is also critical regarding accuracy as well as interpretation of various childhood stuttering research outcomes. For example, studies of natural recovery initiated with children aged 4 and 5 years (e.g., Spencer &_Weber-Fox, et al, 2014; Leech et.al, 2017; Gerwin et al., 2019; Walsh, et al., 2021) can be expected to yield lower, less accurate, recovery rates than those reported by studies initiated when the participating children were of younger age (e.g., Reilly et al., 2009, 2013; Yairi & Ambrose, 1999; 2005). This is so because the considerable number of natural recovery cases that typically occur in 2-3-year-olds will remain unknown, therefore not counted, as well as not addressed, in studies employing older preschoolers; even if only one or two years older.
Furthermore, the sex distribution of the older preschooler is already different. Hence, several clinical predictors for recovery/persistence, such as stuttering severity or using nonwords to form rhymes — two means suggested by Walsh et.al (2021) based on studies of 4-5-year olds, are, most likely, not applicable to 2- year-olds who are just a few weeks or months into stuttering.
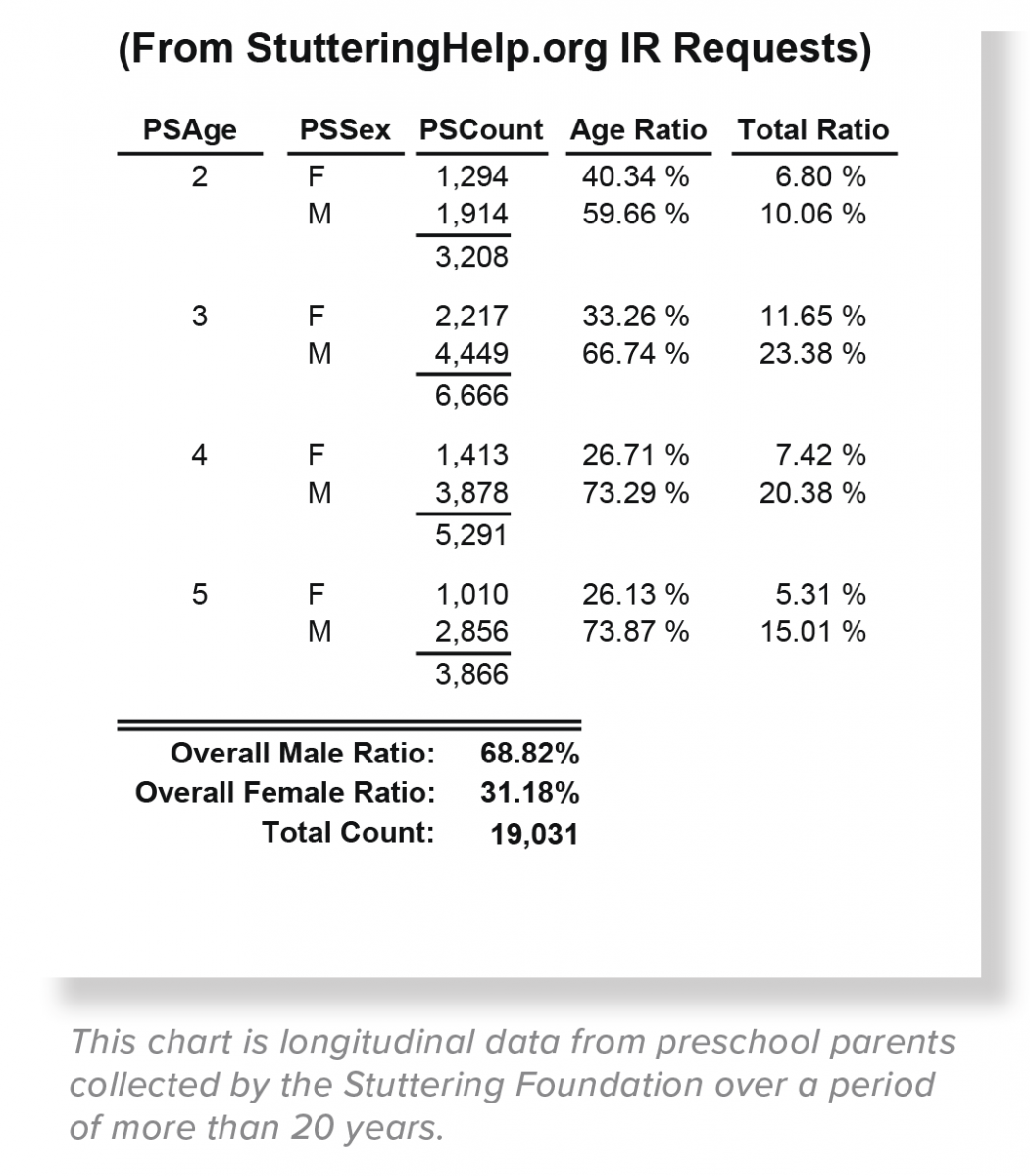
Pertaining to the above is another important age-related phenomenon: the well-known high male-to-female ratio in the stuttering population. Whereas the initial ratio of 2 males to 1 female among 2 to 3-year-old children who stutter (Yairi & Ambrose 1999; 2005), it widens during the sequential preschool years and beyond, eventually reaching to 4/1 or 5/1 (Bloodstein, Bernstein, & Brundage, 2021). Among other consequences, the increased male-to-female ratio as a function of age in experimental child samples consisting of older preschoolers (4 and 5 years of age) lower the real percent of natural recovery as well as affecting other data. Specifically, the older the initial sample of preschoolers, their percent of females is smaller and, therefore, so is the level of their natural recovery. This, in turn, could lead to inadequate predicting factors if/when applied to the younger preschool population as mentioned above.
Yairi and Ambrose (2005) also called attention to the age-related brain phenomenon known as pruning that begins prior to birth and continues during the early years of life. It pertains to nonconductive, or poorly conductive brain neural pathways presenting interferences in the young child's efficient brain functioning that may be reflected in observable difficulties. Could this also pertain to stuttering? These faulty neurons, however, are gradually eliminated, a biological process known as neural pruning. More than 20 years ago, neural pruning was offered by Yairi and Ambrose (2005) as a possible explanation of a biologically-based natural recovery from stuttering.
Finally, important information about persistent stuttering may be uncovered by studying upper age groups — people who have stuttered for many years into advanced ages. Perhaps they exhibit more pronounced characteristics that reveal differences not easily identifiable in the typical child or young adult who stutters. All-in-all, the above notes serve to highlight the role of age in the onset and development of stuttering research, gender distribution, awareness and emotional components, natural recovery data, clinical evaluation and prognosis, and more. Although knowledge is accumulating, much remains to be learned.
REFERENCES
Ambrose, N., & Yairi, E. (1994). The development of awareness of stuttering in preschool children. Journal of Fluency Disorders, 19, 229-245.
Seery, C., Watkins, R., Mangelsdorf, S., & Shigeto, A. (2007). Subtyping stuttering Il: Contributions from language and temperament. Journal of Fluency Disorders, 32, 197-217.
SheikhBahaei, S., Millwater, M., & Maguire, G. A. (2023). Stuttering as spectrum disorder: A hypothesis. Current research in neurobiology. 5, 100116. https: //doi.org/10.1016/j.crneur.2023.100116
Spencer, C., & Weber-Fox, C. (2014). Preschool speech articulation and nonword repetition abilities may help predict eventual recovery or persistence of stuttering. Journal of Fluency Disorders, 41, 32-46.
Walsh, B., Christ, S., & Weber, C. (2021). Exploring Relationships Among Risk Factors for Persistence in Early Childhood Stuttering. Journal Of Speech, Language, And Hearing Research, 64(8), 2909-2927. https: //doi.org/10.1044/2021 JSLHR-21-00034
Watkins, R., Yairi, E., & Ambrose, N.G. (1999). Early childhood stuttering Ill: Initial status of expressive language abilities. Journal of Speech, Language, and Hearing Research, 42, 1125-1135.
Yairi, E., & Ambrose, N. (1999). Early childhood stuttering I: Persistency and recovery rates. Journal of Speech, Language, and Hearing Research, 42(5), 1097-1112.
Yairi, E. & Ambrose, N. (2005). Early childhood stuttering. Austin: Pro-Ed, Inc.