Evaluating Persistence: A Closer Look



Also see: Updated Research Data on Preschool Children
Excerpts from Stuttering: Foundations and Clinical Applications, Third Edition (November 2021, Plural Publishing, Inc.) by Dr. Ehud Yairi and Dr. Carol H. Seery.
In a series of studies conducted by the Purdue University Stuttering Project, data were collected from 52 4- and 5-year-old preschoolers who stuttered and were followed longitudinally.
Initially, the Purdue researchers reported that the clinical assessments with the strongest predictions for eventual stuttering were consonant production abilities and performance on non word repetition tasks (NRT). The children who eventually persisted were less proficient in these two measures than those who eventually recovered. Receptive and expressive language abilities did not distinguish the two groups (Spencer & Weber-Fox, 2014). Later, however, they reported that stuttering children who had steeper productive syntactic growth were more likely to recover (Leech et al., 2017). Next, they reported that children who eventually persisted used non-words to form rhymes (e.g., "blat" to rhyme with "cat") at nearly twice the rate of their normally fluent peers (Gerwin et al., 2019).
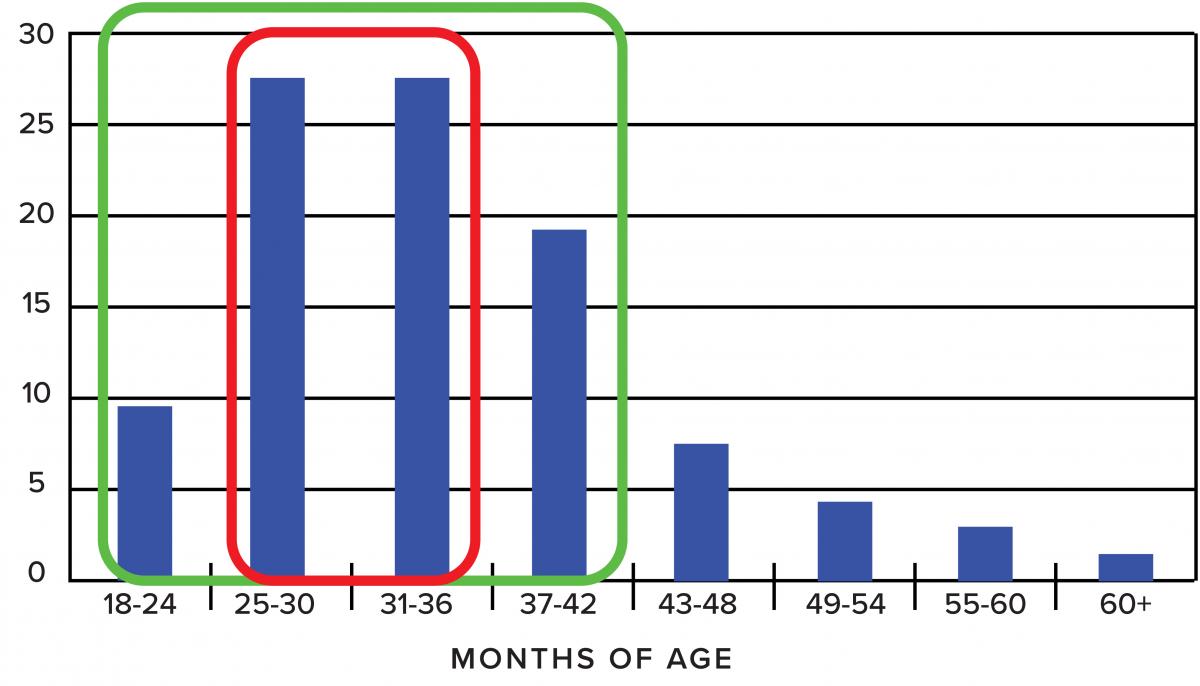 |
| Figure 1 |
The stuttering severity in conversational speech samples of those 4–5 year old CWS revealed that, unlike younger CWS, weighted SLD scores were predictive of eventual stuttering persistence and recovery (Walsh et al., 2020). Finally, the assumption that the relationship among the combined epidemiological and clinical risk factors would yield greater predictive precision than single variables, was examined in the same children. Here, positive family history of stuttering conferred a high risk of persistency. For children who did not have a family history of stuttering, greater frequencies of stuttering-like disfluencies (SLD), lower accuracy on non word repetition (NRT) and poorer articulation abilities, were all associated with an increased probability of persistence (Walsh et al., 2021). These multiple risk factors, they concluded, should result in lower rates of prediction errors (false positive or false negative).
The findings are consistent with the Multifactorial Dynamics Pathways theory of stuttering (Smith & Weber, 2017) that highlights speech-language and motor interaction impacting stuttering persistence (see Yairi & Seery, 3rd ed., chapter 3, for additional information).
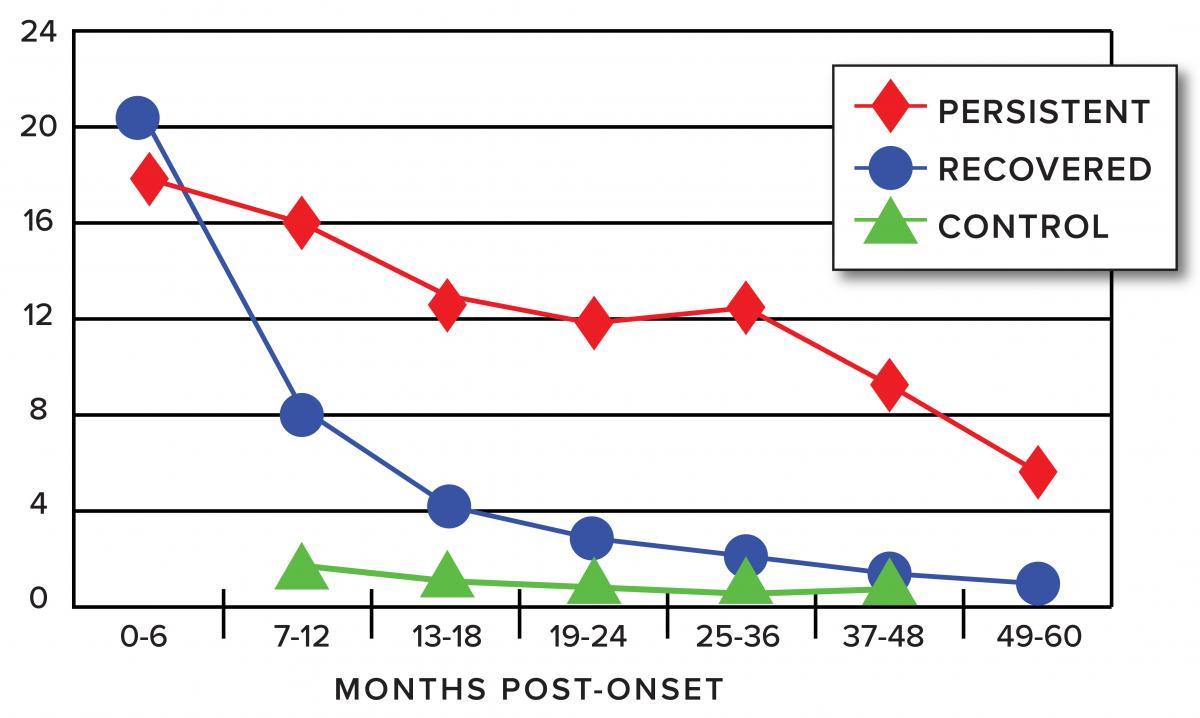 |
| Figure 2 |
Interestingly, some 15 years earlier, the Illinois Project arrived at a similar recommendation concerning the power of applying multiple predictive factors: In reviewing all risk criteria, it become apparent that their predictive power varies and that no single factor has sufficient strength to be relied on as a safe prognostic indicator. To arrive at a meaningful risk assessment, the clinician's task is to thoughtfully examine the combination of criteria as they converge in each individual case. Several examples illustrate different combinations of factors and their interpretations. (Yairi & Ambrose, 2005, p. 355)
The Purdue Project also expanded to brain activity research as indexed by event-related brain potentials (ERPs). Initial findings indicated that their 4–5 year old CWS may exhibit atypical lateralization of ERP for syntactic processing compared to their typically fluent peers (Weber-Fox et al, 2013).
By age 6, however, those who recovered processed syntactic stimuli similarly to NFC whereas the children who continued stuttering displayed a less mature ERPs patterns. Actually, the EPRs patterns of CWS who persisted were more similar to younger (3–5 year-old) typically developing children (Usler & Weber-Fox, 2015).
At ages 7 to 8, children who had recovered from stuttering displayed atypical ERP lateralization over frontal brain areas compared to their NFC peers. Still, even larger differences were noted for the children who persisted in stuttering (Mohan & Weber, 2015). Thus, these studies indicated possible developmental delays in neural function, or altered neural patterns, for those children who persist in stuttering.
Another ERP study of semantic processing in their 5-year-old CWS indicated that those who recovered exhibited more mature patterns compared to NFC and to CWS who would persist (Kreidler et al., 2017). Taken together, these ERP studies indicate that emerging proficiencies in language processing may be subtly altered for CWS and in some cases be related to their recovery or persistency (Smith & Weber, 2017).
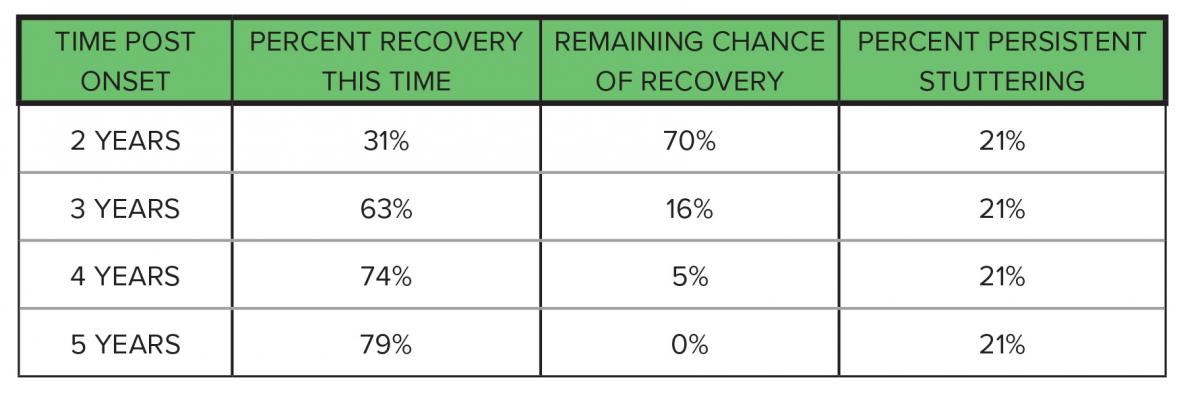 |
| Table 1 |
Important: When comparing the different findings between the Illinois and the Purdue prediction factors, keep in mind the very important differences between their samples of children. The Illinois studies investigated considerably younger children (as young as 24 months of age) who began their participation very close to the onset of the disorder, some within 1 to 8 weeks (mean of 6 months post onset). The Purdue studies of 4- and 5-year olds began with a mean age of 59 months compared with a mean of 39 months in the Illinois project, a nearly two year difference. One of the Purdue reports (Leech et al., 2017) states that the mean children's age when entering the study was 62 months and that the mean age of their reported stuttering onset was 38 months. That is, they were first recorded approximately two years post onset. This is not "close to onset" and the predicting factors can hardly be viewed as "early predictors" (See Figure 1 for age of onset data from the Illinois studies.)
Also, from what the Illinois studies revealed about the rate and timing of natural recovery, it is quite probable that their sample missed about 30% of the potential population of early childhood stuttering, those who recovered during the first two years post onset (see Table 1). This consideration is also evidenced by their low natural recovery of only 44% as compared to nearly 80% when the sample includes younger children close to onset. The more time post onset, the smaller the natural recovery rate.
This means that the Leech et al. (2017) or other studies that employ similar child samples, were already composed of a greater percentage of children with a more robust, resistant form of stuttering as compared to those in a younger sample. We do not doubt the possible validity of their predicting criteria for older children who have stuttered for 2 years or more. We question, however, whether their criteria are applicable to the early months, or even the first year, of the disorder. For example, whereas the Illinois studies found that the level of stuttering (SLD) is not a risk factor during the first 6 to 9 months of stuttering (see Figure 2), Walsh et al. (in press) include this measure as a risk predictor for their older children. Likewise, performance on repeating non words, which they list as a risk predictor, may not be applicable for children who are 24 to 30 months old. Therefore, it seems desirable to consider prediction criteria according to age-specific/disorder duration factors.
Ehud Yairi, PhD, University of Illinois, Professor Emeritus, Speech and Hearing Science
Carol H. Seery, PhD, CCC-SLP, University of Wisconsin Milwaukee, Associate Professor Emerita
From the Fall 2021 Magazine